Administrators: Research
Rationale
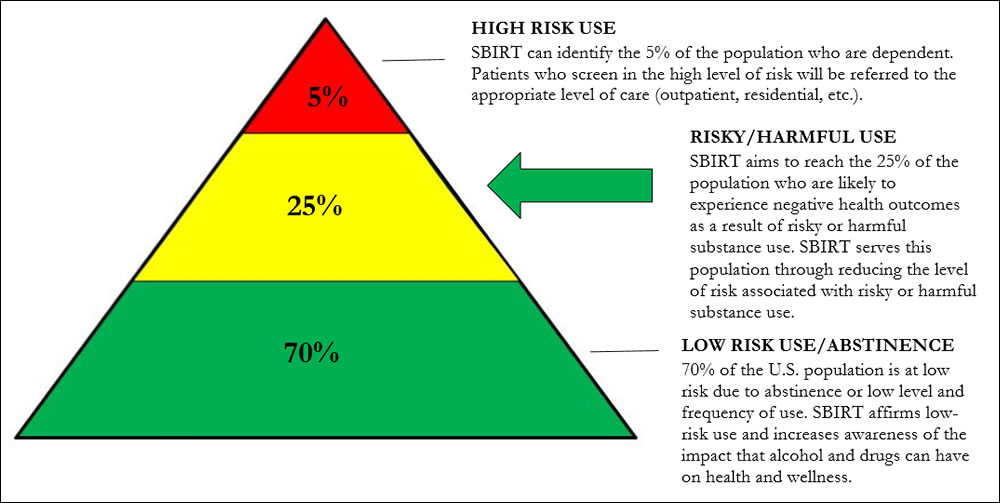
There is a wide range of risk associated with substance use. At one end of the continuum is abstinence and low-risk use; at the opposite end are the risks associated with dependence and binge drinking. While the majority of current programs focus on education and treatment (both ends of the continuum), SBIRT aims to reach individuals who are in the middle of the range of risk.
*For more information on low-risk drinking and effects of harmful alcohol use, click here.
Efficacy
Research has found SBIRT to be effective:
- Heavy drinkers who receive a brief intervention are twice as likely to reduce their drinking as heavy drinkers receiving no intervention.1
- Research has found a reduction of 39% in alcohol use and 68% in drug use, and improved levels of general and mental health at 6-month follow up.2*
* Research findings are mixed on the efficacy of brief interventions on drug use; nevertheless, on-going research continues to expand the current understanding on efficacy.
SBIRT is endorsed by:
- The World Health Organization (WHO)
- The U.S. Preventative Services Task Force
- The Committee on Trauma of the American College of Surgeons
- The Substance Abuse and Mental Health Services Administration (SAMHSA)
Cost Benefit
- The National Commission on Prevention Priorities ranked alcohol screening and intervention 4th on a list of the top 25 preventive clinical services recommended by the U.S. Preventive Services Task Force on preventable burden and return on investment (ROI).3, 4
- Cost-benefit analysis found an 89% cost savings for each patient screened and a $330 cost savings for each patient who received a brief intervention.5
- Reduced health expenditures were $3.81 for every $1.00 spent. If routinely offered to eligible injured adult patients, the potential net savings would be $1.5 billion annually.5
References
- Wilk AI, Jensen NM, Havighurst TC. Meta‐analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12(5):274-283.
- Madras BK, Compton WM, Avula D, Stegbauer T, Stein JB, Clark HW. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. Jan 2009;99(1-3):280-295.
- Maciosek MV, Coffield AB, Edwards NM, Flottemesch TJ, Goodman MJ, Solberg LI. Priorities among effective clinical preventive services: results of a systematic review and analysis. American journal of preventive medicine. 2006;31(1):52-61.
- Solberg LI, Maciosek MV, Edwards NM. Primary care intervention to reduce alcohol misuse: ranking its health impact and cost effectiveness. American journal of preventive medicine. 2008;34(2):143-152.e143
- Gentilello, L.M., Ebel, B.E., Wickizer, T.M., Salkever, D.S., & Rivara, F.P. (2005). Alcohol interventions for trauma patients treated in emergency departments and hospitals: A cost benefit analysis. Annals of Surgery241(4), 541-550.